insights
The Advantages of Facility Data vs. Benchmarking for Staffing Analysis

When it comes to staffing analysis, reports based on actual data from the unique facility––instead of benchmarking––makes all the difference.
Most EVS Directors have experienced this phenomenon: a staffing analysis benchmarking report comes back with the potential for significant savings, if its recommendations are successfully implemented. But in practice, your team struggles to implement those changes without sacrificing quality or service level.
This is a common struggle for EVS Directors, who face the dual challenges of addressing rising HAI rates by cleaning regularly and thoroughly, while also managing the financial and staffing challenges that so many facilities are facing.
That’s why it’s so important to base your decision-making on good data. When it comes to staffing analysis, the difference between what’s theoretically possible and what’s actually doable comes down to basing your reports on your facility’s actual data, instead of statistical calculations based on other hospitals.
The Limitations of Benchmarking
Staffing analyses that rely on benchmarking compare data sets from multiple facilities and use averages to prescribe the level of EVS staff needed per square foot. This can be useful, in terms of giving you a sense of industry norms.
But averages are just that: many facilities have higher staffing levels, and many have lower, based on the unique situation of those facilities. And it’s not just square footage that affects those staffing levels.
There are multiple factors that affect staffing levels beyond just square footage, such as:
- Type of space (what is the mix of office space, ERs, ORs, patient rooms, waiting rooms, etc.);
- Volume of patient room discharges and transfer cleans;
- Patient room census occupancy;
- Management team to employee ratios, as well as the specific responsibilities of management team;
- Public area policing and porter duties (service request responses);
- Paid break time per shift;
- The amount of lock-in areas cleaned such as ER, L&D, NICU, Invasive Radiology, Surgeries, Cath Labs, etc.––areas that need multi-shift EVS attention due to cleaning between cases, or constant turnover;
- Volume of non-cleaning tasks: such as meeting set-ups or supply room stocking.
If, for instance, there are two facilities that both have the same square footage, but one of them has twice the amount of patient rooms, that facility will inevitably need more employee hours to reach the same quality of service and cleaning. And while some of these factors are accounted for in benchmarking numbers, they vary widely by facility, and controlling for all of them is difficult.
There are also other variables to consider when it comes to benchmarking. As with any analysis, you have to make sure that you’re comparing apples to apples. Here are just some of the questions that EVS Directors should consider before relying on benchmarking:
- Are the facilities that this benchmarking report includes similar to your own facility? If your facility is relying on benchmarking, you want to be sure that the facilities those reports are based on are similar to your own when it comes to the factors listed above.
- Do these facilities achieve the level of clean that your facility aspires to? The average HCAHPS rating among US hospitals for cleanliness is 3 out of 5 stars.
- Are these facilities understaffed? The trend in most facilities over time has been a continual decrease in staff in response to hospital budget cuts, so many of the hospitals that benchmarking reports rely on are operating understaffed, and could thus produce artificially low expectations for the hours needed to maintain quality in your facility.
As you can see, benchmarking has a myriad of limitations that can make it difficult for EVS Directors to rely upon it as an accurate staffing analysis tool. But there’s an alternative:
The Alternative: Staffing Analysis Based on Your Facility’s Actual and Unique Data
At Smart Facility Software, we don’t use benchmarks or blueprints to build out the database. Instead, we take an inventory of your facility, so you can analyze your staffing needs based on your unique data.
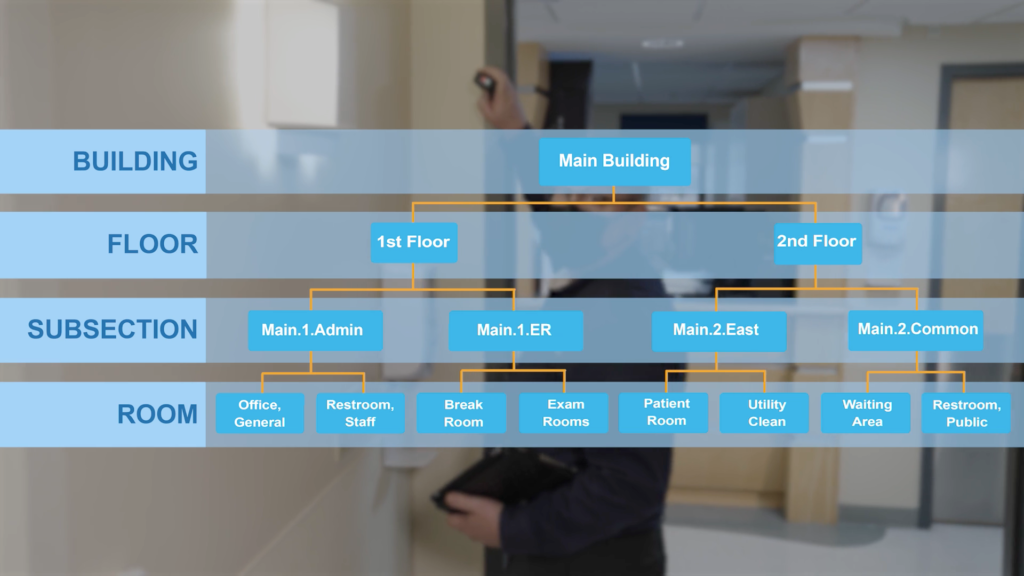
Our EVS consultants literally walk the floors of each hospital facility to determine its scope and specific needs and build a database of rooms and cleaning requirements. Each facility’s database captures not only its square footage, but also factors like the type of space, fixtures in that space, and acuity. In our three decades of service, we’ve recorded over one billion square feet of cleanable area––over twice the size of Manhattan––and that record of each facility’s actual and unique data allows us to adapt the software to your team’s specific needs.
When it comes to staffing calculations, ES Optimizer takes into account your facility’s specific cleaning protocols, as well as other variables and tasks performed by EVS that aren’t related to site inventory, such as lock-ins, waste removal, and non-productive time, among others.
This firsthand knowledge of your facility makes it possible to run staffing analyses and build work assignments that actually meet the needs of your unique facility and budget.